RESEARCH RECORD
The CJC-1295 Research Record
Three decades of GHRH pharmacology, applied to a 30-amino-acid analog with a maleimide linker. Set out feature by feature.
CJC-1295 mechanism of action
How does CJC-1295 work mechanistically?
CJC-1295 is a GHRH-receptor agonist on anterior-pituitary somatotrophs [1]. Binding to the receptor activates Gs-protein-coupled signaling, raises intracellular cyclic AMP, drives protein kinase A activity, and triggers exocytotic release of stored growth hormone. The released GH then acts on hepatic GH receptors to induce IGF-1 transcription [1]. The four amino-acid substitutions in the CJC-1295 sequence — D-Ala at position 2, Gln at 8, Ala at 15, and Leu at 27 — block dipeptidyl-peptidase-IV cleavage between residues 2 and 3, which is what inactivates native GHRH within minutes [6]. The DAC moiety, when present, covalently binds Cys34 of serum albumin via maleimide chemistry; the albumin tether shields the peptide from clearance and extends the plasma residence time by roughly two orders of magnitude [5]. Pulsatility of GH secretion is preserved despite sustained receptor occupancy [2]. The pulse generator is upstream of the receptor and is not desensitized by tonic GHRH-receptor activation across the studied dosing windows.
CJC-1295 with DAC vs no DAC
What is the difference between CJC-1295 with DAC and without DAC?
The two variants share the same 30-residue backbone and the same four sequence substitutions [5]. The DAC variant adds a maleimidopropionic-acid (MPA) lysine derivative at the C-terminus that covalently binds the free Cys34 thiol on circulating serum albumin [5]. The no-DAC variant — equivalent to modified GRF (1-29) — does not. The pharmacokinetic difference is dramatic. CJC-1295 with DAC: plasma half-life of approximately 5.8 to 8.1 days in healthy adults [1]. CJC-1295 without DAC: plasma half-life of approximately 30 minutes. The dosing-frequency implications follow directly: weekly or every-other-week intervals were used in the phase-1 multi-dose arm of the DAC variant [16]; the no-DAC variant requires far more frequent administration in research protocols. The two variants are pharmacodynamically equivalent at the receptor — they bind the same GHRH receptor and drive the same downstream cascade — but produce very different exposure profiles.
Modified GRF (1-29): the precursor to CJC-1295
Modified GRF (1-29) and how it relates to CJC-1295
Modified GRF (1-29) is the 30-amino-acid CJC-1295 backbone without the DAC linker — sometimes written ModGRF, Mod GRF 1-29, or CJC-1295 no-DAC. The four sequence substitutions (D-Ala-2, Gln-8, Ala-15, Leu-27) are identical to those in the DAC variant and confer the same protease resistance [6]. What modified GRF (1-29) lacks is the albumin-binding C-terminal maleimide moiety. In its absence, the peptide is cleared at the rate set by renal filtration and residual peptidase activity, producing a plasma half-life of approximately 30 minutes. Research protocols that prefer pulsatile rather than sustained receptor occupancy use modified GRF (1-29) for that reason. The native unmodified parent fragment — sermorelin / GHRH (1-29) — has a still shorter plasma half-life of approximately 7 to 20 minutes, illustrating how each modification step extends pharmacokinetic residence [10].
CJC-1295 and Ipamorelin: the GHRH + GHRP Pairing
Why CJC-1295 and ipamorelin are studied together
CJC-1295 and ipamorelin activate two non-overlapping receptors on the same target cell [7][8]. CJC-1295 binds the GHRH receptor; ipamorelin binds the ghrelin / GHS-R1a receptor [7]. The downstream pathways are mechanistically distinct: GHRH-receptor stimulation raises intracellular cyclic AMP via Gs; ghrelin-receptor stimulation raises intracellular calcium via phospholipase C and IP3 [8]. Both pathways converge on the somatotroph's GH-release machinery without competing for the same binding site, so combination dosing in published research produces additive — and in some preclinical models supra-additive — growth-hormone pulse amplitude versus either compound alone [8]. Ipamorelin in particular is characterized by selectivity: in healthy-volunteer dose-finding work, dose-dependent GH release occurred without significant elevation of ACTH, cortisol, FSH, LH, prolactin, or TSH [7][15]. That selectivity is why ipamorelin is the conventional GHRP partner for a GHRH analog like CJC-1295 in research protocols where additional HPA-axis activation is undesirable.
CJC-1295 vs ipamorelin: GHRH analog vs GHRP
CJC-1295 versus ipamorelin
These are not the same kind of molecule. CJC-1295 is a 30-amino-acid GHRH analog — a synthetic version of the upstream hypothalamic releasing hormone, acting on the GHRH receptor [1]. Ipamorelin is a pentapeptide (Aib-His-D-2-Nal-D-Phe-Lys-NH2) that mimics ghrelin and acts on the ghrelin / GHS-R1a receptor [7]. Both produce GH release, but through different receptors. The pharmacokinetic profiles diverge as well: CJC-1295 with DAC has a half-life of roughly 7-8 days [1]; ipamorelin is short-acting on the order of an hour in plasma. The two are most commonly described in the research literature as complementary rather than substitutable — pairing them lets researchers stimulate the somatotroph through two independent receptors simultaneously, exploiting the additive pulse amplitude documented across rodent, ovine, and human bolus studies [8].
Effects observed in published CJC-1295 research
Effects observed in published CJC-1295 research
Across the indexed literature, four endpoints recur. Growth-hormone elevation: 2- to 10-fold dose-dependent increases in mean plasma GH following single subcutaneous doses of 30 to 250 µg/kg in healthy adults, sustained at least six days at higher doses [1]. IGF-1 elevation: 1.5- to 3-fold above baseline for 9 to 11 days following a single DAC dose, with cumulative elevation across 49 days in the multi-dose arm at 60 µg/kg weekly or every other week [1][16]. Pulse preservation: pulse frequency unchanged under continuous receptor stimulation; both pulse amplitude and inter-pulse baseline elevated [2]. Downstream proteomic shifts: reproducible changes in serum protein composition following a single 90 µg/kg dose, including downregulation of apolipoprotein A1 and transthyretin isoforms and upregulation of beta-hemoglobin and albumin fragments [4]. These are pharmacodynamic markers — they describe what the molecule does to measurable serum analytes, not what it does to symptoms, body composition, or clinical outcomes in any indicated population.
What clinical and preclinical CJC-1295 studies have reported
What CJC-1295 trials have reported
Two completed phase-1 trials in healthy adults form the published human evidence base for CJC-1295 with DAC: a single-ascending-dose arm (30, 60, 125, 250 µg/kg subcutaneous) and a multi-dose arm (60 µg/kg subcutaneous weekly or every other week for 49 days), with n ≈ 65 total participants across both arms [1][16]. The companion pulsatility analysis [2] used samples from the multi-dose arm. One phase-2 trial of CJC-1295 with DAC in HIV-associated lipodystrophy was halted after a fatal cardiovascular event roughly two hours after the eleventh weekly dose; the trial investigator attributed it to pre-existing coronary disease judged unrelated to study drug, and the development program did not continue past phase 2 [14]. Preclinical work includes the Alba 2006 GHRH-knockout mouse study showing that once-daily CJC-1295 normalized body weight, lean mass, and subcutaneous fat distribution versus untreated knockout controls [3]. The Henninge 2010 analytical-chemistry paper characterized a seized doping-market preparation, confirming the 30-residue sequence and the C-terminal maleimide moiety [5]. The 2025 WADA Prohibited List continues to name CJC-1295 explicitly under Section S2.2 [12].
Onset of measurable effects in published trials
Onset of measurable effects in published trials
Phase-1 trials measured plasma GH elevation within hours of a single subcutaneous dose of CJC-1295 with DAC and sustained IGF-1 elevation for one to two weeks following that single dose [1]. The measured endpoint is biochemical — serum GH and IGF-1 — not subjective. Subjective sensations of energy, sleep quality, or body composition are outside the scope of pharmacokinetic studies and are not reported as primary endpoints in the indexed phase-1 literature.
CJC-1295 and sleep architecture
Does CJC-1295 affect sleep?
Growth hormone is released predominantly during slow-wave sleep, and GHRH-receptor activation has direct sleep-architecture effects independent of peripheral GH. A 1992 study by Steiger and colleagues found that intranasal native GHRH administered 30 minutes before bedtime enhanced slow-wave sleep proportion (particularly in the latter half of the night) and reduced early-night cortisol in healthy male subjects [9]. That work is upstream of CJC-1295 but informs interpretation of any reported sleep observations in the GHRH-analog class; CJC-1295's own published phase-1 trials did not include polysomnography as a primary endpoint.
 FIG. III — VARIANT COMPARISON
FIG. III — VARIANT COMPARISON
| Spec axis | CJC-1295 with DAC | No-DAC variant (modified GRF 1-29) |
|---|---|---|
| Backbone length | 30 residues | 30 residues |
| Substitutions | D-Ala-2, Gln-8, Ala-15, Leu-27 | D-Ala-2, Gln-8, Ala-15, Leu-27 |
| DAC linker | Maleimidopropionic-acid Lys at C-terminus | None |
| Plasma half-life | ~5.8-8.1 days | ~30 minutes |
| Dosing interval (research) | Weekly / every other week | Multiple times daily |
| Receptor target | GHRH receptor (somatotroph) | GHRH receptor (somatotroph) |
Single subcutaneous doses produced dose-dependent two-to-tenfold elevations of mean plasma growth hormone sustained for at least six days and 1.5- to 3-fold elevations of insulin-like growth factor 1 for nine to eleven days. — TEICHMAN 2006 / J CLIN ENDOCRINOL METAB
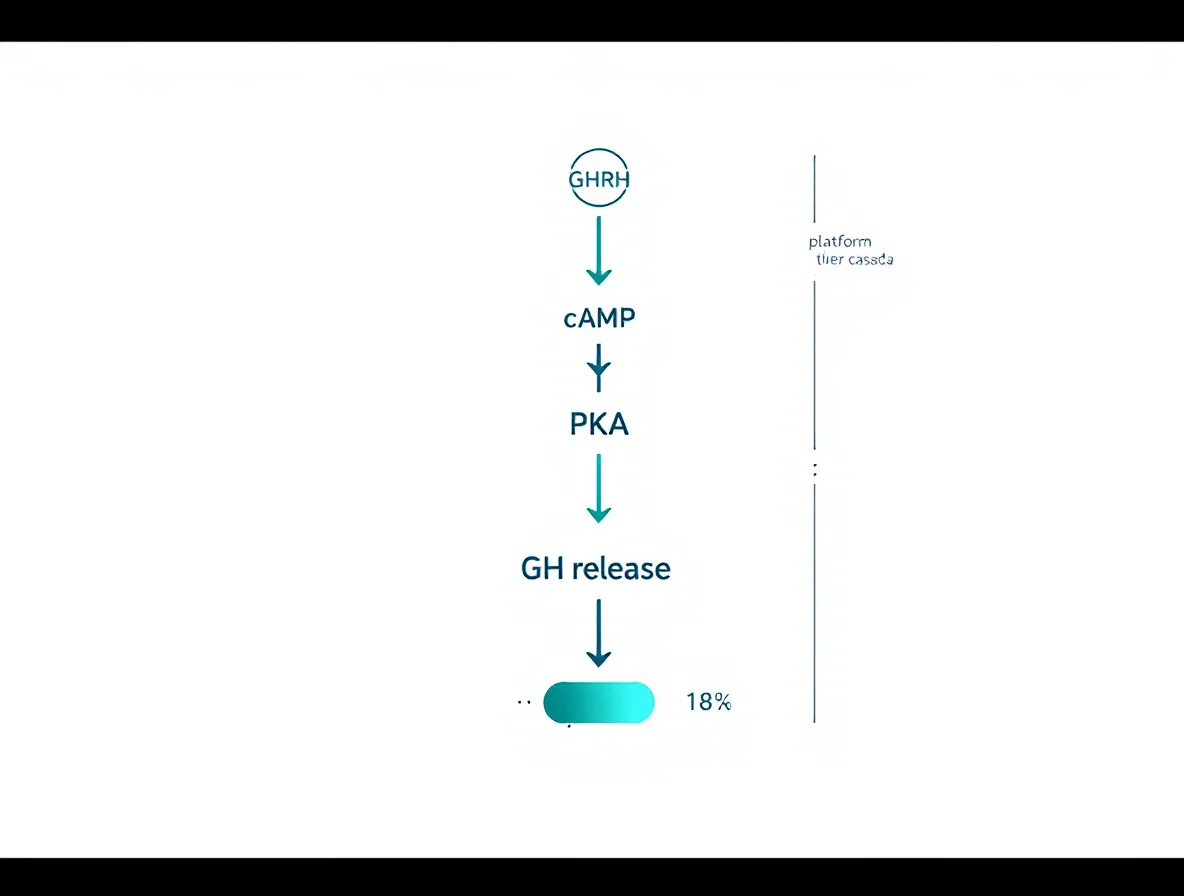 FIG. IV — MECHANISM CASCADE
FIG. IV — MECHANISM CASCADE
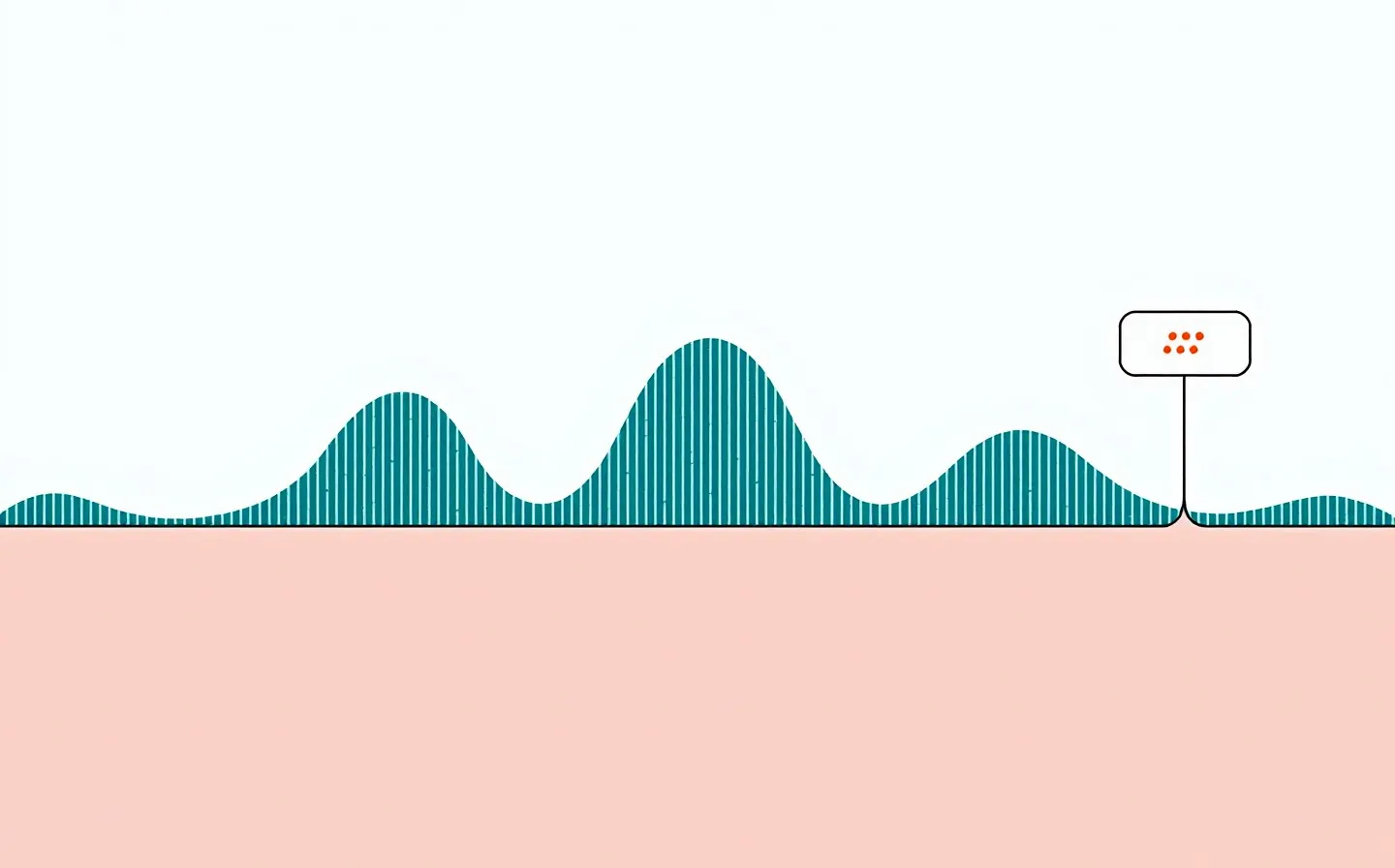 FIG. V — PULSATILE OUTPUT
FIG. V — PULSATILE OUTPUT
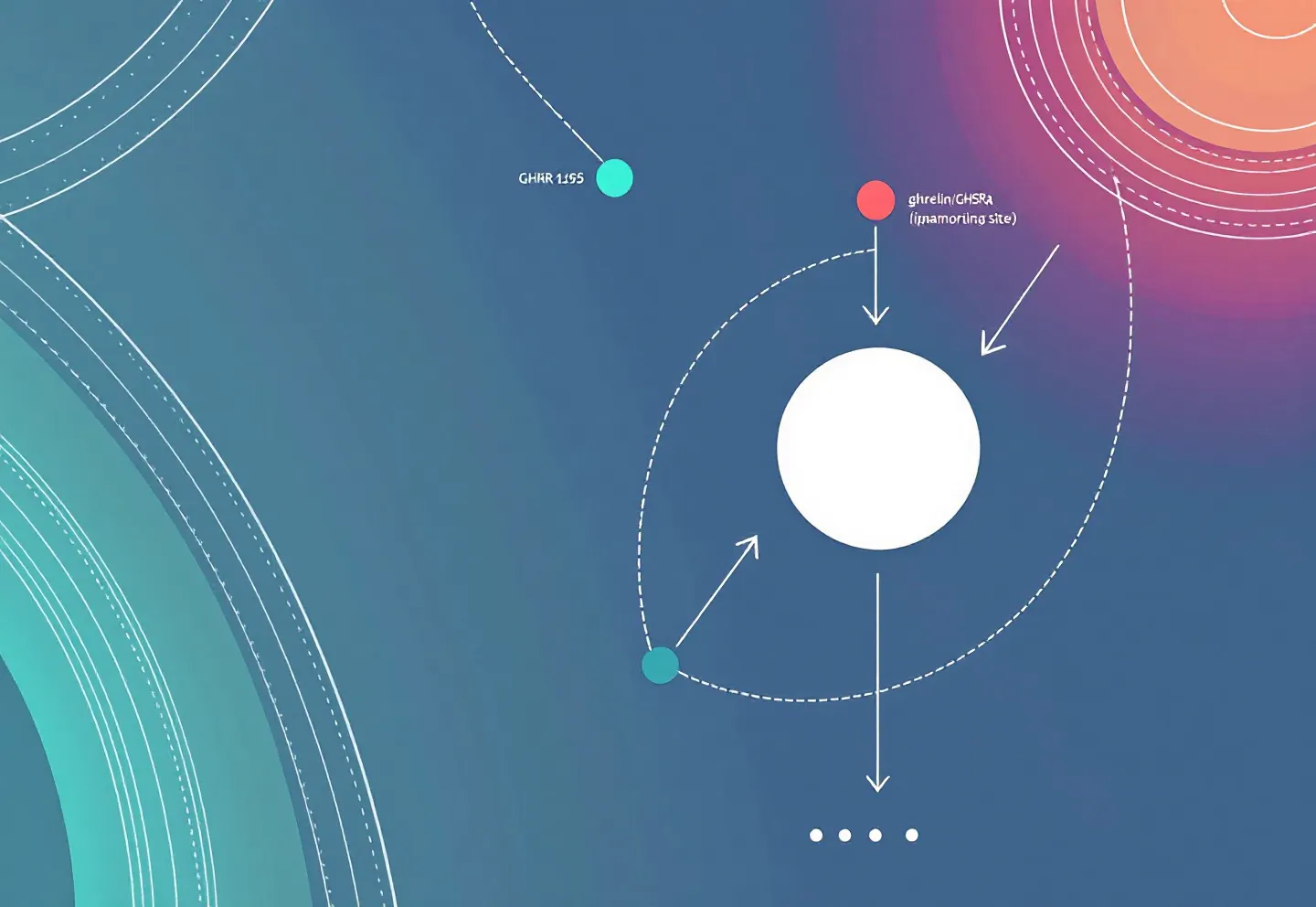 FIG. VI — RECEPTOR PAIRING
FIG. VI — RECEPTOR PAIRING